
Traditional Chinese Medicine Is a Modern Invention
How “Obsolete Medicine” became “Chinese,” and what happened everywhere it traveled

I avoided acupuncture for decades. I trust a study over a story, and the needles always seemed like something to be polite about, not something to try. Then last winter my neck seized up. A friend pushed me toward acupuncture (针灸, zhēnjiǔ), and I finally went.
The doctor put a needle in my forehead, not my neck, somewhere above the brow. Within a few minutes my neck loosened. I still have no good account of why.
I grew up with Chinese medicine the way most Chinese families do, as herbs and medicine, boiled bitter soups from a TCM (Traditional Chinese Medicine) doctor prescription/recipes. That was Chinese medicine to me: something you drank, not something that was done to your body.
The other surprise came from the doctor herself. She was from Taiwan, learnt TCM there, but practicing fully licensed in a neighborhood public hospital in Shanghai. A Taiwan doctor holds a Chinese state license to practice in a mainland public hospital.
Old Medicine Needed a New Enemy
Before China met Western medicine, there was no need for a category called “Chinese medicine.” There was just medicine, 医 (yī). The compound 中医 (zhōngyī, “Chinese medicine”) means something only against 西医 (xīyī, “Western medicine”). A tradition acquires the name only when a rival shows up to make it look local.
In February 1929, fourteen men met in Nanjing 南京 (then capital of China) to decide the future of Chinese medicine. None of them practiced it.
They were the first National Public Health Committee (中央卫生委员会) of the new Nationalist government. Most were Western-trained physicians, returnees from Japan, Europe, and America, brought in to build a modern medical system. The doctors who actually treated the overwhelming majority of Chinese patients, the practitioners of 旧医 (jiùyī, “obsolete medicine”), were not invited.
The physician Yu Yunxiu (余云岫, 1879–1954) put a proposal before that room. Yu was Japan-trained. He had already written 《灵素商兑》, a book-length attack on the founding classics of Chinese medicine. His proposal’s title left nothing to interpretation: 《废止旧医以扫除医事卫生障碍案》, A Proposal to Abolish Old Medicine in Order to Sweep Away the Obstacles to Public Health. His argument was not purely medical:
旧医一日不除,民众思想一日不变,新医事业一日不能向上……为民族进化计,为民生改善计,不可不取断然手段,此乃国家大计。
So long as the old medicine survives a single day, the people’s thinking will not change, and the enterprise of new medicine cannot rise… For the nation’s evolution, for the people’s welfare, decisive measures must be taken. This is a matter of state.
Chinese medicine was condemned not as ineffective but as a way of thinking, a leftover of the pre-modern mind that a modernizing nation had to clear away. The needle and the herb were incidental. The target was a worldview.
And the committee did not move to ban it. It moved to register it to death. The measures were procedural. Registration of old-style doctors would close at the end of 1930. Old-medicine schools would be banned. The press would be cleared of it. A practitioner over fifty might receive a “special license,” but he would be barred from treating infectious disease or signing a death certificate, and the license would expire in fifteen years. No books burning in a square. Just a registry set to close, schools that could never open, and a generation of old doctors holding permits with an expiry date. Chinese medicine was not to be killed. It was to be allowed to die of old age, on a schedule, certified by a form.
Then the plan leaked. It surfaced first in Shanghai’s newspaper, then in triumphant detail in Yu’s own journal, and the press named it the 废止中医案, the Abolish-Chinese-Medicine Bill.
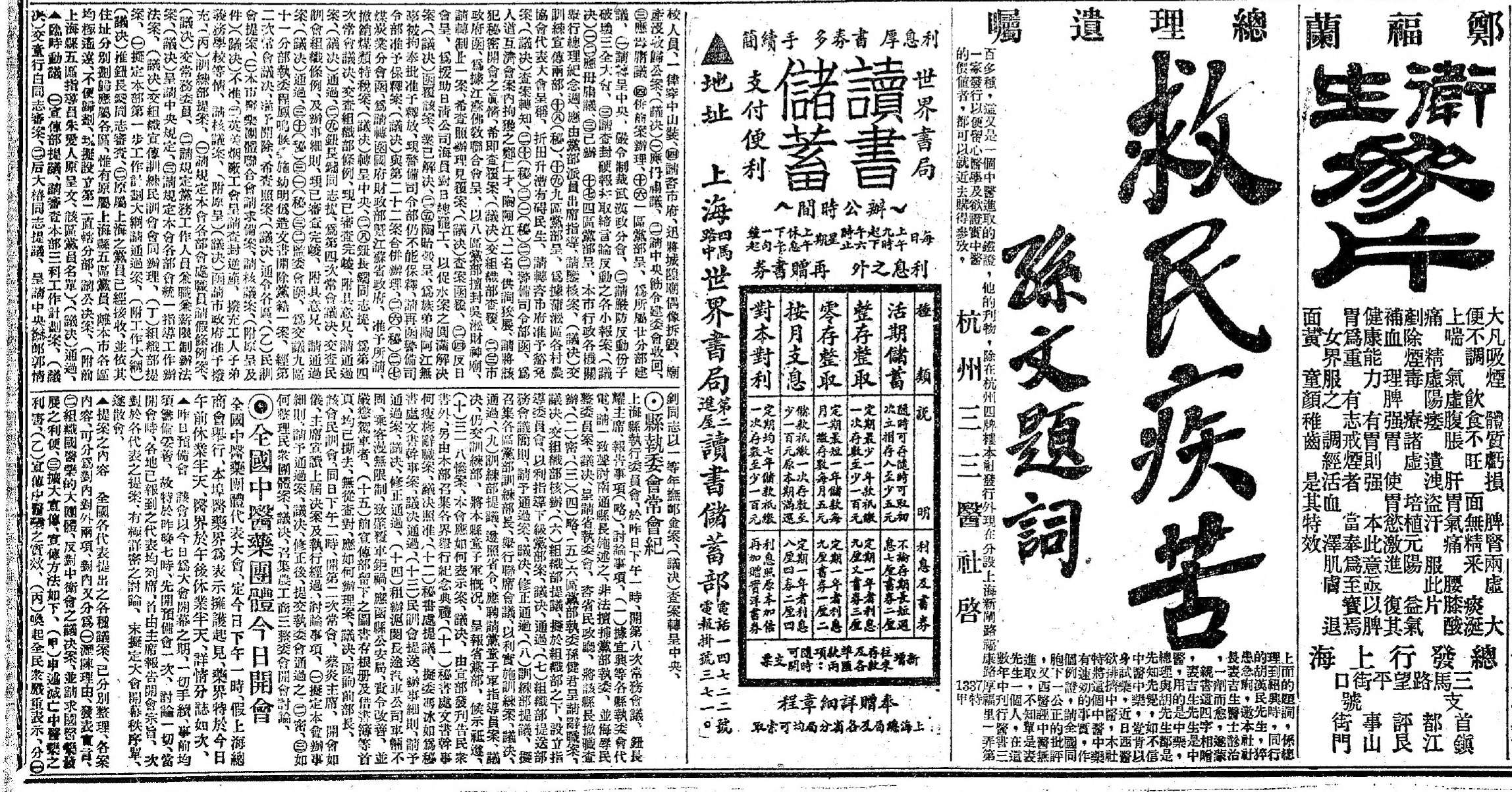
Practioners went furious. Shanghai’s practitioners shut their clinics by the thousand and packed more than forty associations into a single hall. They resolved to build a standing body and to convene a national congress. On March 17, 1929, delegates from Chinese-medicine associations across fifteen provinces filled the great hall of the Shanghai General Chamber of Commerce (上海总商会). The city’s pharmacies made it a public event. The great houses, 胡庆余堂, 蔡同德堂, 达仁堂, closed for half a day and hung banners across their fronts.
拥护中医药,就是保持我国的国粹。取缔中医药,就是致病民的死命。
To defend Chinese medicine is to preserve the nation’s essence. To outlaw Chinese medicine is to sentence the sick to death.
The operative word is 国粹 (guócuì), the “national essence.” In three weeks the defenders had turned a quarrel about medicine into a referendum on China itself. The journal 医界春秋 tied abolition to imperialist aggression, linking the survival of the medicine to the honor of the nation. It was the same nationalism Yu had aimed at them, turned back the other way.
And it worked. The major papers, 申报 Shun Pao chief among them, covered the protest with sympathy. The petition delegation took the train to Nanjing and found the government softer than its own committee had been. The premier, Tan Yankai, declared flatly that Chinese medicine absolutely cannot be abolished. The bill was shelved. March 17 became 国医节, National Medicine Day, the holiday marking the day Chinese medicine saved itself.
To avoid being registered out of existence, Chinese medicine had to become the one thing it had never been: a single, governable, modern entity the state could sit across a table from. Its enemies drew the blueprint.
What Was Actually Invented
In 1929, then, Chinese medicine learned to act as one body politically. It was not yet one body intellectually.
“Old medicine” was not a system. It was a library and a guild rolled together over two thousand years, competing lineages, regional schools, rival theories that contradicted one another, transmitted master to disciple with no fixed curriculum and no central authority deciding who was right. The historian Nathan Sivin describes the inheritance not as a tradition but as a “myth of an unchanging medical tradition”1 laid over two millennia of a medical system in turmoil. There was no single doctrine called Chinese medicine, because there had never needed to be one.
The single doctrine was built in the 1950s, in under a decade. The new state had perhaps half a million traditional practitioners and only ten to twenty thousand Western-trained doctors. A vast population needed care, and the cheap, abundant resource was the old medicine. So the state set out to make it usable, which meant making it uniform. Committees, often led by Western-trained physicians with traditional doctors as advisers, took the sprawling, contradictory inheritance and carved out of it a single internally consistent system, one that could be taught from a textbook and would not embarrass the language of modern science.
In 1956, the State Council established the first four colleges of Chinese medicine in Beijing, Shanghai, Guangzhou, and Chengdu. It was the moment informal apprenticeship became standardized higher education. The first textbook, 《中医学概论》 (Outline of Chinese Medicine), was written in Nanjing in 1958. A full set of eighteen unified national textbooks was finished by 1962. Even the bedrock concept now sold as the timeless core of the medicine, 辨证论治 (biànzhèng lùnzhì, “pattern differentiation and treatment”), the idea that the practitioner treats a syndrome-picture rather than a named disease, was elevated and codified in exactly this period, lifted from the variety of older practice and installed as the defining method of the whole field.
The standardization was efficient. It was also lossy. Rival lineages, regional variations, minority-tradition remedies that did not fit the approved framework. These were not banned, but they were no longer taught. What the committees produced was a clean, teachable, internally consistent system. What it cost was the mess, and the mess had been where much of the medicine’s local diversity lived.
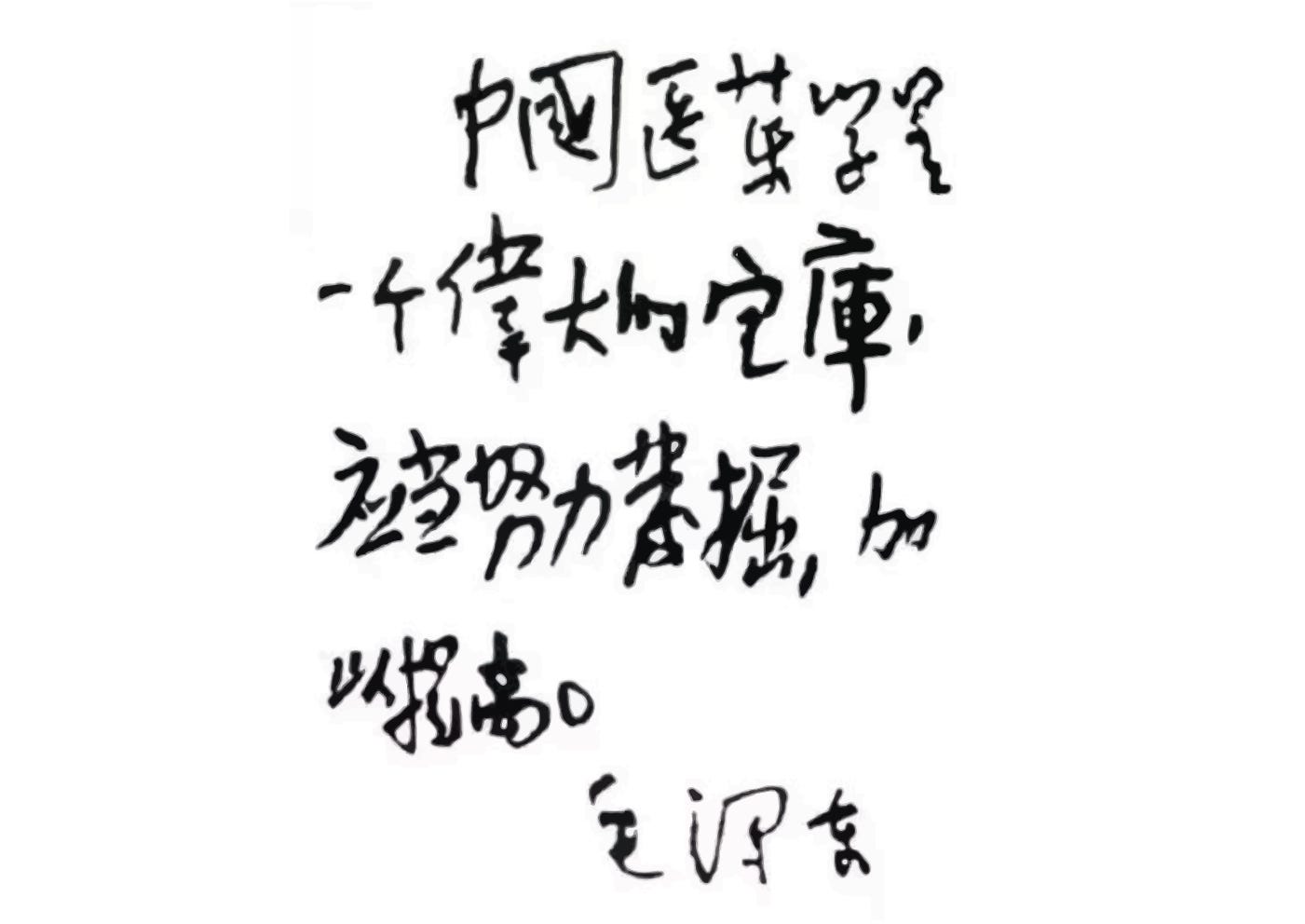
Mao was an advocate, in his own calligraphy, that still runs across the front of TCM publications: 中国医药学是一个伟大的宝库, Chinese medicine and pharmacology are a great treasure house. The phrase did real work. It reframed what the 1929 reformers had called a pre-modern obstacle as a national asset, a “treasure-house” to be mined by modern science, not swept away by it. And the English name itself was part of the construction. The term “traditional Chinese medicine” was coined by party propagandists around 1955. It was a label produced, in English, for a system being built in Chinese.
What was invented was the system: the claim that these scattered, contending practices form one coherent medicine, with a unified theory, a standard curriculum, a national set of textbooks, a degree, and a name. “Traditional Chinese Medicine” is the brand the People’s Republic printed, in the 1950s, on a tradition it had just finished standardizing. The tradition is real. Its unity is manufactured. And once a thing has been standardized into a single exportable system, it can be shipped. And of everything in it, one piece traveled farther than all the rest: the needle.
The Needle That Crossed the Ocean
In 1971 the New York Times columnist James Reston had an emergency appendectomy in Beijing. Acupuncture was used to manage his post-operative pain, and his front-page account introduced the practice to America. What China then advertised to the visiting West was “acupuncture anesthesia,” patients awake through major surgery, anesthetized by needles alone. In May 1972, two traditional doctors (Pien Bae Chi 卞伯岐 & Leung Kok Yuen 梁觉玄) gave a public demonstration in San Francisco before some five hundred American physicians. That same year California began moving to regulate the practice; in 1976 it became one of the first states to license acupuncturists. Today some forty-seven states regulate acupuncture, often as a credential separate from herbs entirely.
The system the PRC had spent the 1950s assembling, almost none of it boarded the plane. What crossed was the needle. The West licensed acupuncture, not Chinese medicine. A practitioner can be certified to put the needles in and never touch the diagnosis, the herbs, the cosmology. The West received a fragment and licensed the fragment.
“Acupuncture anesthesia” was a spectacle, and like many spectacles of the Cultural Revolution it does not survive scrutiny. Western anesthesiologists who examined acupuncture anesthesia later concluded that the “success” owed less to the needle than to heavy pre-operative coaching, careful patient selection, and the political pressure of the moment. Acupuncture anesthesia quietly disappeared. What survived was a narrower, sturdier claim: that the needle relieves pain. A real science grew up around it.
For half a century, scientists have looked for the mechanism behind acupuncture, endless effort to render 气 (qì) and 经络 (jīngluò, the meridians) into molecules. In the 1970s the physiologist Han Jisheng (韩济生) and others showed that acupuncture’s pain relief could be blocked by naloxone. That implicated the body’s own opioids. They also found that different needling frequencies released different neuropeptides.2 In 2010 a team at Rochester found that acupuncture raises adenosine in the local tissue, and that without the adenosine A1 receptor the pain relief disappears.3 More recently, Qiufu Ma’s lab traced how stimulating a defined set of nerve fibers at a specific point can drive a vagal anti-inflammatory reflex, a neuroanatomical reason why one point might genuinely differ from another.4 And in 2025 a UCLA group did the thing no one had managed. They collected cells from the tip of an acupuncture needle in a human point and sequenced them, reporting a previously uncatalogued cell population that expanded as the patient’s pain receded.5
Despite a great deal of research into what lies behind the needle, the practice of acupuncture still largely operates within a standardized traditional framework of yin and yang, organ systems, and pattern differentiation. The Foundations of Chinese Medicine, one of the best-selling English-language textbooks on Traditional Chinese Medicine, was written by Giovanni Maciocia, who trained at the Nanjing University of Chinese Medicine — the same Nanjing institution involved in producing the PRC’s first standardized TCM textbooks in the late 1950s.
The Only Textbook in the Room
In the mainland itself, the system that was standardized in the 1950s now runs on two tracks. The main path is the one built on those colleges: a five-year university degree followed by the national TCM Practicing Physician Qualification Exam (中医执业医师资格考试). But the 2017 law went further. It formally preserved the apprenticeship path. A practitioner who has studied under a qualified master for five years, with two licensed TCM physicians vouching for him, can sit a practical assessment before an expert panel and receive a license to practice his specific specialty. No university degree required. The state that standardized everything also kept a door open for the older way of learning.
The investment has always been political as much as medical. Officials are evaluated partly on TCM adoption metrics in their districts. During COVID-19, provincial governments promoted traditional formulas as a national alternative, a “Chinese solution,” with a fervor that owed as much to political performance as to clinical evidence. The result is a system backed by enormous state resources, research funding, and institutional weight. It also shaped, at every level, by the needs of the state that funds it.
In Hong Kong, herbal medicine is older than the colony itself. Ko Shing Street (高陞街) in Sheung Wan has been the center of the herbal trade since the late nineteenth century. Walk it today and pass shopfronts where dried seahorses hang beside sliced deer antler, where ginseng roots are sorted by grade behind glass, where the air is sweet and medicinal and has been for over a hundred years. These shops were built on Cantonese folk knowledge, on southern Chinese remedies passed down through families and guilds, on a practitioner class that had no national curriculum. Acupuncture here was practiced the same way, learned in clinics, passed teacher to student, with no standardized point chart on the wall.
Then came the ordinance. In 1999 Hong Kong required every Chinese-medicine practitioner to register. The territory’s universities built degree programmes, and when they needed a curriculum, the one available, the one already written into textbooks and organized into courses, was the mainland’s. The acupuncture training, the herbal pharmacopoeia, the diagnostic framework, all now taught from the same standardized system.
Singapore’s story runs even deeper, and through a different channel. Chinese medicine there was never a national tradition. It was a clan tradition. When Hokkien, Teochew, Cantonese, and Hakka immigrants arrived in the nineteenth century, they brought their own regional remedies, their own dialects, their own doctors. The Thong Chai Medical Institution (同济医院), founded in 1867, offered free consultations and medicine to the poor, decades before any standardized “Chinese medicine” existed anywhere. Eu Yan Sang 余仁生 opened its first Singapore shop in 1910, serving migrant workers who could not afford Western doctors, and its name means “caring for mankind” in Cantonese. These were community institutions, rooted in dialect and kinship, not in a unified theory of 辨证论治.
When Singapore’s government registered them all under the Traditional Chinese Medicine Practitioners Act in 2000, it imposed a single frame on a patchwork, and it started with the needle. Acupuncturists were registered first, from 2001; physicians followed from 2002.
When Nanyang Technological University launched its TCM degree in 2005, the degree was conferred by Beijing University of Chinese Medicine. For twenty years Singapore’s only university-level TCM diploma carried Beijing’s name. NTU announced in 2024 that it would finally issue its own degree starting in 2028. The health minister’s phrase was telling: stand on its own two feet.
Same Classroom, Different Diploma
A TCM student in Taipei and one in Beijing open the same books. The 《伤寒论》Treatise on Cold Damage Disorders, the 《黄帝内经》The Yellow Emperor’s Inner Canon, the pattern-differentiation framework, the organ-system theory, the canonical acupuncture point categories, the core curriculum is, for all practical purposes, the same. Taiwan’s universities have quietly used mainland textbooks as references for decades. The theory taught on both sides of the strait traces back to the same 1950s codification. The political wall and the textbook market do not run on the same map.
And yet the credentials do not cross. Taiwan does not recognize mainland medical degrees. Its own license is famously demanding: from the 1980s a seven-year college programme, and in 2011 the closing of the 中医师特考, the special examination that had let self-taught and apprenticed practitioners qualify. That was the master-disciple route by which most of postwar Taiwan’s renowned physicians, herbalists and acupuncturists alike, had earned their standing. The apprentice was not outlawed. It was de-licensed out of existence. The mainland, in the same period, preserved exactly that path.
The asymmetry runs the other way too. Since 2007 the People’s Republic has built specific channels for Taiwan physicians to obtain mainland medical licenses, by examination, or, for senior doctors, by direct recognition. Chinese medicine is explicitly one of the permitted categories. These rules sit on the websites of the offices for Taiwan affairs as much as the health ministry. The mainland recognizes Taiwan training. Taiwan does not return the gesture.
Which is where my Shanghai clinic comes back. My doctor studied TCM in Taiwan, sat the mainland’s exam, and now practices in a neighborhood public hospital. The same textbooks, the same theory, the same needle. Nothing about the medicine changed when she crossed. What changed was the license on the wall.
If my insights brought you a fresh perspective, please consider supporting me by buying me a coffee. Your generosity fuels my writing.
Science and Medicine in Imperial China — The State of the Field https://www.jstor.org/stable/2056359
Han, J. S. (2004). “Acupuncture and endorphins.” Neuroscience Letters, 361(1–3), 258–261. DOI: 10.1016/j.neulet.2003.12.019. PMID: 15135942.
Goldman, N., Chen, M., Fujita, T., Xu, Q., Peng, W., Liu, W., Jensen, T. K., Pei, Y., Wang, F., Han, X., Chen, J.-F., Schnermann, J., Takano, T., Bekar, L., Tieu, K., & Nedergaard, M. (2010). “Adenosine A1 receptors mediate local anti-nociceptive effects of acupuncture.” Nature Neuroscience, 13(7), 883–888. DOI: 10.1038/nn.2562. PMID: 20512135.
Liu, S., Wang, Z., Su, Y., Qi, L., Yang, W., Fu, M., Jing, X., Wang, Y., & Ma, Q. (2021). “A neuroanatomical basis for electroacupuncture to drive the vagal-adrenal axis.” Nature, 598(7882), 641–645. DOI: 10.1038/s41586-021-04001-4. PMID: 34646018.
Yu, X., et al. (2025). “Single-cell transcriptomic analysis reveals dynamic changes of the cellular composition of acupuncture point BL23 (Shenshu) in low back pain.” Molecular Pain, 21. DOI: 10.1177/17448069251405974. PMID: 41312958. (Published online ahead of print, November 28, 2025.)
Like everything you write, this is such a fascinating history - thank you! The creation of TCM during the consolidation you describe seems like a textbook (no pun intended) example of institutionalization creating knowledges, something like Foucault might have said about European Enlightenment contexts. But I also feel that this kind of story gets co-opted sometimes by anti-acupuncture polemicists, like those who responded to the recent NYTimes article about the interstitium's similarities to meridians. I saw some claiming that the theory and practice itself - not just the governmental system - was invented in the 20th century. Some even suggested that there actually was no acupuncture before then, because there wasn't steel to make needles. It would be really interesting to expand or follow up on this piece with a dive into that classical medicine history in a way that debunks that kind of over-simplification and maybe adds the next level of nuance to this history you're telling here. Not that Substack is a place for people to drop requests, but . . . :)
One of the most interesting pieces I’ve read on Substack so far, thank you!